SEND August 2025
Special Educational Needs and Disabilities (SEND)
Find links to useful resources, webinars and podcasts to support children in relation to SEND
- Safeguarding and SEND
- 4 main areas of SEND
- Neurodiversity
- Neurodiversity protective factors
- ADHD explained
- Online safety for SEND
- Mythbusting
- Executive Functioning
- Co-occuring problems
- ADHD Resources
- Non-verbal communication
- Non-verbal resources
- SEND one minute guides
- SEND resources
- Signposting to Services
Safeguarding & SEND
Safeguarding children with SEND is everyone's business and is not the sole responsibility of specialist teams. We take a partnership approach to safeguarding all children regardless of their vulnerabilities.
Children with SEND may have:
- additional needs
- additional support for learning
- additional learning needs
Being aware of the added vulnerabilities that SEND children may encounter will help you to better protect them.
Some children may have additional vulnerabilities because they:
- have additional communication needs
- do not understand that what is happening to them is abuse
- need intimate care or are isolated from others
- are dependent on adults for care

What are the different areas of SEND?
There are 4 main areas of need:
- Communication and interaction: This area covers difficulties with speech, language, and non-verbal communication, as well as challenges in understanding social cues.
- Cognition and learning: This includes children who learn at a slower pace than others, have difficulties with understanding, memory, and organisation, or struggle with literacy and numeracy. This might also include learning difficulties such as dyslexia or dyspraxia and other cognitive difficulties
- Social, emotional and mental health difficulties: This area addresses difficulties in managing relationships, anxiety, withdrawing from social situations, or other challenges with social, emotional, and mental health
- Sensory and/or physical needs: This includes difficulties with sensory processing (like sight or hearing) and various physical impairments or disabilities that affect a child's ability to access facilities and carry out daily activities.

Neurodiversity
Understanding Neurodiversity
Neurodiversity means that people’s brains work in different ways and that’s completely natural. Instead of viewing these differences as problems or disorders, neurodiversity celebrates the variety in how people think, learn, and experience the world.
Conditions like ADHD, Autism, Dyslexia, Dyspraxia, Dyscalculia, Tourette’s Syndrome, and Dysgraphia are all part of neurodiversity. People with these differences often have unique strengths, such as creative thinking, pattern recognition, problem-solving, and attention to detail.
However, many environments aren’t designed with neurodiversity in mind. By creating inclusive spaces and showing understanding, we can help neurodivergent individuals thrive and feel valued.
Why Neurodiversity Awareness Matters in Safeguarding Children
For practitioners working to safeguard children, understanding neurodiversity is vital. Neurodivergent children may express themselves, behave, or react to situations in ways that differ from neurotypical expectations. Without awareness, these differences can be misunderstood or overlooked, potentially putting children at risk.
Being neuro-aware helps practitioners to:
By embedding neurodiversity into safeguarding practice, professionals can better protect children’s wellbeing, promote trust, and create safer environments where every child feels understood and supported.
-
Understanding diversity within neurodiversityShow detailsKey:
-
Neurodiverse children can be more at risk in safeguarding contexts for several reasons.Show detailsKey:
-
Flexible approachesShow details[ADD LINKS]
Training for professionals in education, health, and social care to better understand neurodiversity.
Clear communication tools like visual aids, social stories, and person-centred planning.
Early intervention and diagnosis to ensure children get the support they need.
Safe environments that respect sensory needs and offer predictable routines.
Practitioners need to be mindful that some parents of children who are neurodiverse, may have neuro diversities of their own. Being aware of this and adapting your approach may assist in gathering information and building relationships.
Identifying strengths as a protective factor for safeguarding
Identifying strengths in children with neurodiversity can help to safeguard them from harm and abuse
We know that children who experience neurodiversity are more at risk than neurotypical children as they have an over trusting nature and need a little extra help to safeguard them from harm. Understanding how a neurodiverse child perceives the world and what they need to keep them safe from harm is an essential blueprint to effective safeguarding.
How to reduce risk
- Inclusivity reduces stigma and promotes acceptance many children and adults with neurodiversity have low self-esteem which can lead to people pleasing behaviour, sometimes risk taking behaviour might look like 'fitting in' to a child, be that from a positive or negative environment.
- Access to tailored resources access to sensory-friendly spaces gives a child a chance to calm the mind when in overwhelm, visual aids help to process, and flexible routines help accommodate diverse needs
- Unique cognitive abilities many excel in creativity, pattern recognition, empathy, long term memory and a unique perspective (which can make them excellent problem solvers) as well as hyper focus on areas of interest
- Self-awareness understanding their own strengths and abilities will empower them to know how to communicate their needs, worries and fears without fear of rejection (see rejection sensitivity dysphoria which is common for most people with ADHD). Knowing that there isn't something 'wrong' with them prevents mental ill health.
- Coping strategies Techniques like mindfulness, structured routines, and sensory regulation can help to reduce anxiety and burnout. Allowing a child to recognise their own patterns establishes good techniques for the future
- Early identification and intervention can prevent isolation, misunderstandings and escalations of low self-esteem as well as academic struggle
We know that many challenges neurodiverse children face often comes from inaccessible environments and rigid expectations and not from the child themselves. Be mindful to not to expect a neurodivergent child to fit into a neurotypical world.
ADHD explained
Find out everything you need to know about Attention Deficit Hyperactivity Disorder (ADHD) in children.
ADD/ADHD is not a behaviour problem. It has far more to do with the brain’s management system. Thomas E. Brown, PhD, discusses ADHD diagnosis, ADHD symptoms and reminds us that ADHD has nothing to do with how intelligent a person is.
Online safety
Neurodivergent children may need a different approach to keep them safe, especially online as they can be more vulnerable to abuse and self-neglect. Reporting abuse can also be a challenge.
THE NSPCC partnered with Ambitious about Autism to bring online safety tips, advice and activities specifically for parents and carers of children with SEND.
Visit the NSPCC online safety pages here or the WSCP staying safe online page here and the Speak Up Stand Up Child Exploitation online safety advice here

-
Show details
 All ADHD children are hyperactive False
All ADHD children are hyperactive FalseStudies show that typically boys can present as more physically hyperactive than girls but hyperactivity can also occur in the brain activity and can often be internalised.
Recent findings suggest there isn’t necessarily a ‘deficit’ in attention in so much as in ‘self-awareness’ and is better described as attention dysregulation (as there are tidal surges in brain activity). Many children with ADHD can become hyper focussed on certain tasks if they are engaged and enthusiastic about the content or subject matter.
-
Show details
 ADHD is more common in boys False
ADHD is more common in boys FalseADHD can present as hyperactive (internal and external) impulsivity and inattentive (more likely experienced by girls), this has led to an underdiagnosis of girls with ADHD as masking and mimicry is more common in girls.
-
Show details
 ADHD is caused by bad parenting False
ADHD is caused by bad parenting FalseADHD is a difference in neurotypical brain activity, not a behavioural problem. Many parents are not aware their child has ADHD and are unsure, like many practitioners, of how to put coping strategies in place to deal with some of the challenges their child may face. 1 in 4 children have a parent with diagnosed or more likely, undiagnosed ADHD and the other 3 out of 4 are likely to have a more distant family member with ADHD.
This assumption ignores the biological impact of ADHD and perpetuates the stigma around neurodiversity.
-
Show details
 Children with ADHD are lazy False
Children with ADHD are lazy FalseThis statement undermines the challenges that neurodiverse children face on a daily basis.
The opposite is in fact true; many will suffer with overwhelm which can lead to executive brain dysfunction – an inability to maintain focus for a long period of time, indecision paralysis which can look like procrastination and ‘laziness’, poor time management and organisational skills.
-
Show details
 ADHD children just need to focus more False
ADHD children just need to focus more FalseADHD is not a choice. Some of the ‘variety’ in neurological brain activity will not allow a child to ‘focus’ through choice. If an ADHD child is in an environment of stress, either in the home, through transitions or at school they will experience the world differently to a neurotypical child.
Other problems may exacerbate this challenge, such as poor sleep, poor nutrition and mental ill health as well as hormonal fluctuation in girls which can lead to increased cognitive difficulties, irritability, distraction and depressive episodes.
-
Show details
 ADHD does not exist False
ADHD does not exist FalseADHD was recognised in 1902 but references date back to the 18th century. In 1902, knowledge around this area was limited to an awareness that there was an issue with hyperactivity in some young boys that could not sit still.
It was seen as a behavioural issue of boys rather than a brain management or difference in executive functioning in any child / adult. Historically much of the research has been carried out on white Caucasian males which would explain the disparity of race and gender ADHD diagnosis.
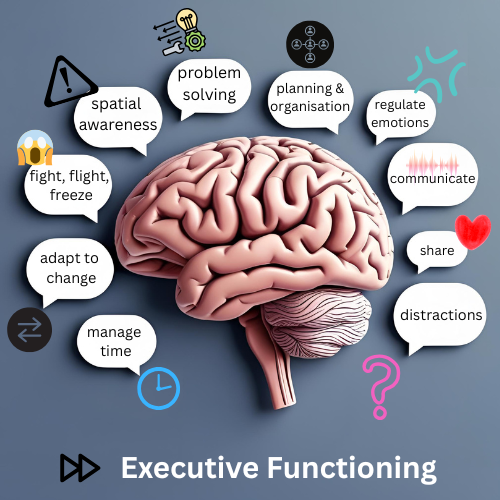
What is Executive Functioning
...and how does it affect a neurodivergent child?
Executive functioning controls the mental skills that help us manage time, stay organised, regulate emotions, and complete tasks. These skills are crucial for navigating everyday life and they often show up differently in neurodivergent individuals.
Executive dysfunction isn’t about laziness or lack of motivation. It’s often rooted in neurological differences, developmental factors, or trauma. Misunderstanding these challenges can lead to stigma or misdiagnosis, especially when someone appears “high functioning” in other areas.
It is extremely difficult for a child with neurodiversity to do many things that a neuro typical person would take for granted and can range from any, many or all of the following:
- short term memory - can be difficult when retrieving information for exams for example or remembering appointments and recall of expectations, tasks and pertinent points from lessons or conversations. Many will have too many thoughts, ideas, feelings to process at once; sometimes described as feeling like a 'computer virus in the head' which is taking up too much space
- difficulty staying focussed - listening for a long time without being distracted by noise, textures, smells, intrusive thoughts or ideas (they may need to communicate these straight away before they lose track of thoughts). Switching between tasks or adapting to change can be harder, especially for those with autism or ADHD
- emotional dysregulation - it may be hard for a child to push overwhelming feelings or ideas to one side without them becoming intrusive, catastrophising events, or overreacting to perceived threats such as criticism or being ignored. Frustrations can become all-consuming if they aren’t recognised and dealt with
- hypervigilance or hyperactivity (internal or external) - a child who does not have a stable home and who feels unsafe may be in a constant state of hypervigilance / hyperactivity
- regulation of sleep - poor sleep through an overactive mind, nutrition and anxiety can be a catalyst to overwhelm and burnout, which can perpetuate the a cycle of negativity that many unsupported children find it impossible to get out of
- managing actions - may look like restlessness, difficulty in changing pace - either speeding up or slowing down, risk taking, keeping quiet and time management
Remember executive dysfunction is not a choice. A neurodiverse child will likely be battling with many issues quietly, without your awareness and sometimes their own. Transitional changes, sudden changes such as loss and grief, divorce and abuse will have a huge impact on the neurological functioning of a neurodiverse child. If a child is undiagnosed these problems can be greatly exacerbated, particularly by hormonal fluctuations.
-
Show details
Autism (+ADHD = AuDHD) Autism is a neurodevelopmental condition characterised by deficits in three main areas: social communication, social imagination and social interaction, with sensory sensitivities also being present.
AuDHD can lead to unique challenges and experiences for individuals diagnosed with both, to find out more visit here
-
Show details
Anxiety & Mood Disorder 3 in 10 children with ADHD also experience an anxiety disorder. Anxiety can manifest in various ways in children, and when it co-occurs with ADHD, it can present unique challenges. Here are some common signs and symptoms of anxiety in children:
Excessive worrying or feeling ‘on-edge’
Restlessness or difficulty sitting still
Trouble sleeping, or experiencing nightmares
Avoidance of certain situations or activities
Physical symptoms like headaches or stomach aches
Being easily startled, or having a heightened startle response
Difficulty concentrating or focusing due to worryEarly support is essential especially when external factors in the home and academic stresses are present as they will greatly exacerbate these symptoms.
-
Show details
 Eating DIsorders Individuals with ADHD, generally girls, face a heightened risk for eating disorders, most notably bulimia nervosa and binge eating disorder, according to a growing body of research. Eating disorders appear to grow in severity alongside ADHD symptoms.
Eating DIsorders Individuals with ADHD, generally girls, face a heightened risk for eating disorders, most notably bulimia nervosa and binge eating disorder, according to a growing body of research. Eating disorders appear to grow in severity alongside ADHD symptoms.Several factors – biological, cognitive, behavioural, and emotional, may explain why ADHD predisposes individuals to eating disorders and challenges. Understanding these factors, including the relationship between a patient’s ADHD and eating disorder, is essential when devising an appropriate and effective treatment plan. Visit here for more information
-
Show details
 Substance Misuse / Addictions People with ADHD are at a higher risk of developing SUD (Substance Use Disorder) and is more prevalent in males. This may be because impulsivity and inattention associated with ADHD can lead to experimentation with drugs and alcohol. If a child is unsafe and at risk of harm this is much more likely and can lead to problems later in life.
Substance Misuse / Addictions People with ADHD are at a higher risk of developing SUD (Substance Use Disorder) and is more prevalent in males. This may be because impulsivity and inattention associated with ADHD can lead to experimentation with drugs and alcohol. If a child is unsafe and at risk of harm this is much more likely and can lead to problems later in life. -
Show details
 OCD ‘Obsessive-compulsive Disorder’ is a disorder related to anxiety. OCD is characterised by two main components: obsessive thoughts and compulsive behaviours.
OCD ‘Obsessive-compulsive Disorder’ is a disorder related to anxiety. OCD is characterised by two main components: obsessive thoughts and compulsive behaviours.There are many overlapping symptoms, or behaviours, between Autism and OCD such as
Compulsive-like behaviours
Restricted and repetitive behaviours
Fixation on routines
Ritualised patterns of behaviour
Resistance to change
Restricted interests -
Show details
 Self-Harm For children that are hypo-sensitive, self-harm may be present. Children may be seeking an input of sensory stimulation because they don't understand their emotions, it can be a way of avoiding total shut down in their body. If you see a child with bruises, it may mean they have self-harmed due to hypo-sensitivities. For example, if a child has been taken into care, they may self-harm to express their emotions.
Self-Harm For children that are hypo-sensitive, self-harm may be present. Children may be seeking an input of sensory stimulation because they don't understand their emotions, it can be a way of avoiding total shut down in their body. If you see a child with bruises, it may mean they have self-harmed due to hypo-sensitivities. For example, if a child has been taken into care, they may self-harm to express their emotions.
ADHD / Autism Resources
A day in the life of a child with ADHD
Short animation explains ADHD through the eyes of amazing ADHD'er Molly
Aimed at school children to help them understand the condition beyond the misconceptions that most adults have these days.
How To Spot ADHD In 'Kids' & The Link Between ADHD and Crime
PODCAST. Sarah Templeton is a passionate advocate for adolescents and adults with ADHD
She has seen the catastrophic effects of the condition not being diagnosed early enough. Her decades volunteering and working with the homeless, serving & ex-offenders and with addicts had flagged up the disproportionately high amounts of ADHD in these groups; who have such an easily treatable condition which had been allowed to destroy their lives. Purely because nobody including teachers, CAMHS, GPs, probation, the police and prison services and charities working in the sectors haven’t spotted it.
-
 Understanding and supporting my child's ADHD Booklet for parents
Understanding and supporting my child's ADHD Booklet for parents -
 Teenagers and ADHD Booklet for teenagers
Teenagers and ADHD Booklet for teenagers -
 The ADHD hero Activity book
The ADHD hero Activity book -
 Find out morePost it note recall to enable more accurate timelines of events in ASD interviewing autistic witnesses and victims
Find out morePost it note recall to enable more accurate timelines of events in ASD interviewing autistic witnesses and victims



Non-Verbal Communication
Connecting emotions
It is important to remember that when a child is non-verbal it does not mean they do not understand nor that they cannot communicate at all. It is the job of the professionals supporting to understand the child’s chosen method of communication and use this (where possible). Often, non-verbal children can be intelligent beyond their years but haven't found their voice, so exploring other ways to communicate without words is essential. Non-verbal children, as well as other children on the spectrum, generally struggle with connecting their emotions. Emotional overload can cause a physical shut down which they may not be able to understand.
There are many tools that can be used to encourage communication such as flash cards and colouring books which explore the use of colour to explain emotions.
A child may be verbal in one setting and non-verbal in another, such as at home when feeling safe but become non-verbal at school when they are overstimulated, or a mixture of both, depending on their emotional state. This is generally known as selective mutism. Providing a safe space for a child will allow them to process what is going on for them at that time and be able to communicate this with a trusted adult when they are ready.
If a child has been abused, providing a picture such as a body chart / silhouette may help the child to communicate where they are feeling an emotion or where in their body, they have been hurt. Building trust with a non-verbal child is essential in keeping them safe from harm.

Developmental Language Disorder (DLD)
2 children in every average classroom of 30 have DLD
These difficulties create barriers to communication or learning in everyday life and aren’t due to another condition.
Lots of children have it, yet most people don’t know about it.
The Silent Child
Produced by Slick Films
A deaf 6-year-old girl named Libby lives in a world of silence until a caring social worker gives her the gift of communication.
-
Show details
 Non-verbal APP: PECSTalk™ The PECSTalk™ app can be used to make requests, respond to questions, comment and ask questions. By converting pictures and text into spoken language, the PECSTalk™ app empowers non-speaking learners to fully participate in their school, home, vocational, and community settings. The app’s digital display is similar in layout to a traditional PECS Communication Book while accommodating the more robust vocabulary of a Speech Generating Device (SGD).
Non-verbal APP: PECSTalk™ The PECSTalk™ app can be used to make requests, respond to questions, comment and ask questions. By converting pictures and text into spoken language, the PECSTalk™ app empowers non-speaking learners to fully participate in their school, home, vocational, and community settings. The app’s digital display is similar in layout to a traditional PECS Communication Book while accommodating the more robust vocabulary of a Speech Generating Device (SGD). -
Show details
 Non-verbal APP : CommBoards Lite AAC Assistant The app helps children and adults of all ages who struggle with speaking find their voice.
Non-verbal APP : CommBoards Lite AAC Assistant The app helps children and adults of all ages who struggle with speaking find their voice.
Clear Communication: The app is perfect for those with Autism, Aphasia, Apraxia, ALS, Motor Neuron Disease, Cerebral Palsy, and Down Syndrome.
Complex Care Needs
Children with complex care needs often require a coordinated approach from agencies such as health, education, and social care.
Safeguarding these children is particularly important as their increased vulnerability, due to physical, cognitive, or emotional challenges, can heighten risks of neglect, abuse, or exploitation. It demands a proactive, multi-agency approach that prioritises their voice, ensures consistent monitoring, and addresses both their medical and emotional well-being.
Practitioners should remain vigilant to signs of harm that may be masked by their care needs, advocating for environments that are not only safe but also nurturing and inclusive.
Sometimes, however, what may look like neglect or harm may not actually be the case. Interventions may need to be put in place to help the parent of a child with complex health needs cope better with every day life. If you have any worries or concerns, speaking to the complex care team as well as other agencies may be all that is required to better safeguard a child.
- Complex care team click here for more information
- Short breaks info click here for information
- Training [link ppt slides]

-
Show details
Communication Barriers Many children with complex needs have speech, language, or cognitive impairments that make it difficult to express concerns or describe abuse.
They may not understand that what is happening to them is wrong or abusive. -
Show details
Dependency on Adults These children often rely on multiple carers for intimate personal care, increasing the number of adults with unsupervised access to them.
Their dependency can make it harder to resist or avoid abuse, especially if they are physically or cognitively impaired. -
Show details
Isolation and Limited Social Networks Children with complex needs are more likely to be socially isolated, with fewer trusted adults or peers to confide in.
They may be excluded from mainstream education or activities, reducing opportunities for others to notice signs of distress. -
Show details
Misinterpretation of Behaviour Signs of abuse (e.g., withdrawal, aggression, regression) may be wrongly attributed to the child’s condition rather than seen as indicators of harm.
Practitioners may overlook safeguarding concerns due to over-identification with the challenges faced by parents/carers.
Changes in behaviours can often be a sign that something is wrong and may be the only sign of communication you get from a child and should be noted. Practitioners who know children well can often spot these subtle changes that need to be investigated. -
Show details
Limited Access to Safety Education Many children with complex needs may not receive accessible education about relationships, boundaries, and personal safety.
This lack of awareness could make them less able to recognise or report inappropriate behaviour.Professionals can use the following resource Private Parts Song |These Are My Private Parts | Body Safety Song by Ollie | Songs for Toddlers to communicate boundaries in a simple but meaningful way.
-
Show details
Parental Stress and Carer Burnout Caring for a child with complex needs can be emotionally and physically exhausting, increasing the risk of neglect or abusive behaviour from overwhelmed carers.
In some cases, parents may also have additional needs that affect their capacity to provide safe care.
Short breaks may support at this time as well as referring to other targeted / universal services if appropriate. -
Show details
Medical Vulnerabilities Frequent medical procedures and medication use can lead to risks such as misuse, unnecessary interventions, or neglect of medical needs.
Children may be at risk of fabricated or induced illness (FII), where a caregiver exaggerates or causes health problems.
Safeguarding Best Practices
To protect children with complex health needs, professionals should:
- Listen to the child’s voice, including non-verbal communication.
- Ensure accessible education on safety and relationships.
- Maintain professional curiosity, don’t assume behaviours are just part of the child’s condition.
- Work closely with families and multidisciplinary teams to monitor wellbeing.
- Provide extra pastoral support and safe spaces for disclosure.

SEND one-minute guides
explore these one-minute guides when working or volunteering with children with SEND in their family.
- 1MG Neurodiversity
- 1MG Short Breaks
- 1MG Safeguarding deaf children
- 1MG SENDIASS - Special Educational Needs and Disabilities Information Advice Support Service
- etc
- etc
- etc

SEND Resources
for more information in SEND take a look at the following booklets, guides, videos, podcasts, policies and more
Wakefield Local Offer
The SEND Local Offer is something every Local Authority has to have.
The Wakefield local offer is a resource for parents, carers and professionals. Visit Wakefield SEND Local Offer | Wakefield SEND Local Offer for more information.

SEND Signposting
-
Beat AutismVisit Beat autism
Wakefield service, offering 1-1 support for parents and children living with Autism as well as training and workshops for schools. Training will enable being able to see things through the eyes of an Autistic child, understanding how the child perceives the world and why they ‘behave’ as they do and ultimately how to change that behaviour. Kids clubs also available in the local area.
-
Down's Syndrome Support Groupvisit the website
A volunteer led local service for parents and professionals offering useful resources and local information such as events and groups.
-
KidzawareVisit Kidzaware website
Offering educational programmes, training and consultancy for all children and adults with a disability
-
Special Education Needs & Disability ServicesDownload resource
For a more comprehensive list of services, both nationally and locally, download the PowerPoint presentation with links to education specific support, information for siblings, funding and much more.
-
Wakefield Parent Carer ForumWakefield Parent Carer website
An independent parent carer forum in April 2020 run by local parents. The forum is run by a group of parents who are passionate about making a positive difference to improve the quality of life for SEND families in Wakefield. Find out information on grants, short breaks, advice, access resources and more by clicking on the button.
-
WESAILWESAIL SENDIASS website
Wakefield Early Support, Advice, Information & Liaison Service A confidential service that covers Pre and Plus Working Support as well as Wakefield’s Local Offer, empowering individuals through the provision of information, advice, support and signposting on a variety of matters including education, health, social care, and leisure.
-
WISSENDSSWISSENDSS resource
Wakefield Inclusion Special Educational Needs and Disabilities Support Service has qualified, experienced teachers and support staff, who have all undertaken extensive training and gained additional qualifications in the educational needs of children with Special Educational Needs and/or Disabilities (SEND). This team of specialists' support at all levels to enhance professional knowledge, skills and expertise based on the national and local education needs identified by schools for children and young people aged 0-25 years. This service is available to schools within the Wakefield District by emailing WISENDSS@wakefield.gov.uk.
-
WISSENDSS ConnectWISSENDS leaflet
https://www.wakefieldparentcarers.co.uk/UserFiles/File/LA_Documents/WISENDSS-Leaflet-PDF.pdfWakefield Inclusion Special Educational Needs and Disabilities Support Service also has a a parent support helpline called WISSENDSS' Connect. Signposting parents to local services and local support as well as any SEND queries they may have.
-
 Local Contacts
01924 302465 or email:
Local Contacts
01924 302465 or email:
sengroup@wakefield.gov.ukFor all SENART queries
-
 Complex Care Needs Team enquiries 01924 302124
Complex Care Needs Team enquiries 01924 302124
or for school admissions / school transport call 01924 305619
Support in Wakefield